Source: Next Steps in Derm
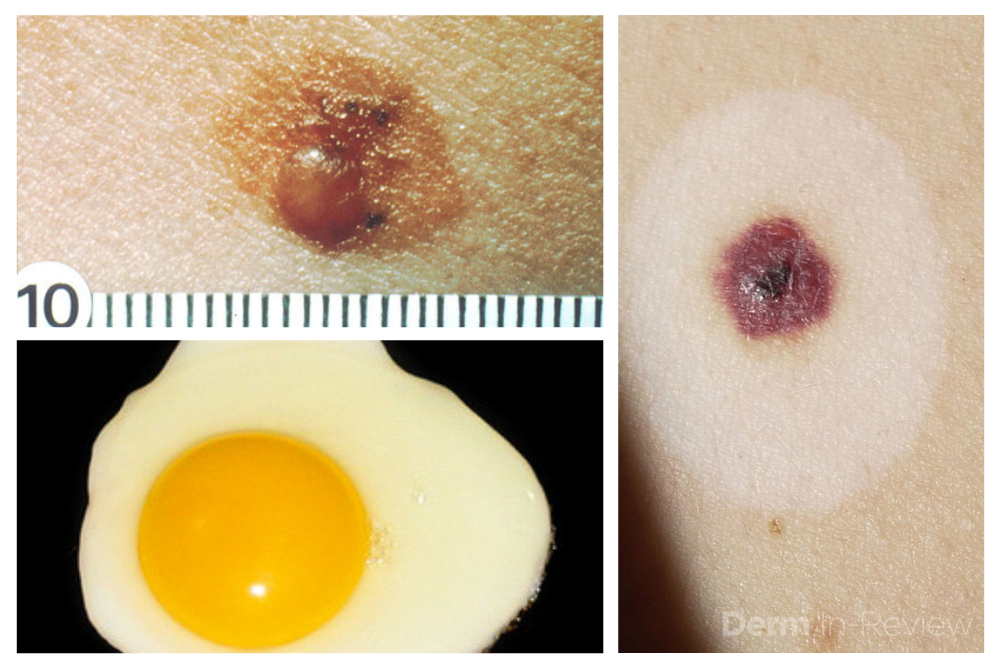
Dermoscopy, also known as epiluminescence microscopy, epiluminoscopy or skin surface microscopy, is an important way to visualize subsurface structures in the epidermis and dermis. In a 2-part series, Dr. Sima Jain reviews the evaluation of pigmented lesions, and the different vessel morphologies and patterns along with a discussion of specific findings in select cutaneous infections.
Read part 1 here
Read part 2 here
If you want to learn more about dermoscopy, make sure to register for the upcoming ODAC Dermatology, Aesthetic & Surgical Conference where Dr. Sima Jain will lead the following dermoscopy sessions:
The Utility of Dermoscopy in Challenging Clinical Cases
During this session, Dr. Jain will present challenging clinical cases and explore how dermoscopic evaluation can significantly increase clinical acumen.
Attendees will:
- Learn how to use dermoscopy to help differentiate types of alopecia
- Learn how to use dermoscopic features to differentiate between melanoma and pigmented basal cell carcinoma
- Learn the dermoscopic features seen in cutaneous lupus and other rashes with follicular plugging.
PEARL ALERT!
Perifollicular scaling and fibrotic white dots are seen in lichen planopilaris. Orthogonal white streaks can be seen in melanoma. Glomerular vessels are often seen in Bowen’s disease.
Dermoscopy Essentials for Residents & Practicing Physicians
During this session, Dr. Jain will review the basics of dermoscopy and how it can be used to help diagnose both pigmented and non-pigmented skin lesions.
Attendees will:
- Learn how to correlate the colors seen on dermoscopic exam with histopathology.
- Learn how to distinguish non-melanocytic growths from melanocytic growths.
- Learn how to use vessel morphology to help diagnose cutaneous malignancies.
PEARL ALERT!
White streaks can be seen in melanoma and basal cell carcinoma. Telangiectasias, leaf-like areas and spoke wheel pigmentation are seen in basal cell carcinomas. The delta wing jet with contrail is specific for scabies.